| Congenital Heart Defects - Pulmonary Atresia with Intact Ventricular Septum (PA-IVS) |
| Hypoplastic Right Ventricle & Tricuspid Valve, Atrial Septal Defect
|
|
What’s wrong?
- There are various spectrum of this condition
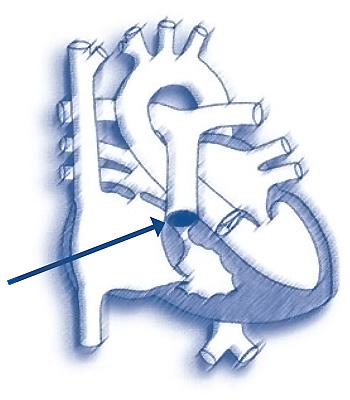
- Usually Pulmonary valve is atretic (not formed) and Ventricular Septum is intact (i.e. no communication between right and left ventricles)
- Blue Blood (Deoxygenated Blood) cannot flow from the RV into the PA and on to the lungs
- At birth, they rely on PDA
- As PDA starts to get small, Oxygen Saturation can drop. Most time, doctors will start Prostin infusion (to keep PDA open) shunt is inserted
- The RV size vary – normal to hypoplastic
Corrective Procedures?
This condition can only be corrected with open heart surgery.
- Soon after Birth
- Modified Bhalock-Taussig Shunt (MBTS)
Create a shunt between the systemic and pulmonary arteries that may help increase blood flow to the lungs e.g. Right MBTS - right subclavian artery to right pulmonary artery – using synthetic graft ( Gore Tex 3 – 4 mm) – this will maintain Oxygen Saturation of more that 80%. The baby will be pink with this saturation.
- Complete repair depends on the size of the Pulmonary Arteries (PA) and Right Ventricle (RV)
6-9 months of Age (9-10 kg)
- if Pulmonary Arteries and Right Ventricles are of good size - suitable for Biventricular Repair
- Take Down of BT shunt and insertion of conduit (tube) connecting Right Ventricle to Pulmonary Artery using Tube graft with valve inside or Homograft
If the RV is small and deemed not suitable for biventricular repair
- May need to go towards Univentricular Pathway ( Fontan Pathway)
- Bidirectional Cavo Pulmonary Connection (BCPC) at approximately 10 kg
- Total Cavo Pulmonary Connection (TCPC)/Fontan Procedure – 2-3 years old
| |
|